Slide batches fail for reasons that are not always obvious, and pathology laboratory water is rarely the first variable investigated. The staining protocol is sound, the reagents are within specification, and the instrument has passed its daily checks. Yet contaminated or poorly controlled water sits upstream of every one of these failure modes.

Ionic residues, organic compounds, microbial byproducts, and particulate matter can each compromise a diagnostic workflow before any staining or amplification step begins.
A dedicated water system controls these variables at source. Without one, a laboratory is managing water quality reactively, after the results have already been affected.
Water Quality as a Pre-Analytical Variable in Pathology
Most pre-analytical error controls in a pathology laboratory focus on specimen handling, fixation timing, and reagent lot tracking. Water rarely appears on that list.
Yet every buffer preparation, every wash step, and every reagent reconstitution introduces water directly into the analytical pathway, which means its quality is subject to the same controls as any other laboratory input.
How Contaminants Reach the Analytical Pathway
Water carries four categories of contamination that matter in a diagnostic context. Ionic contaminants (dissolved mineral salts and charged particles) alter buffer conductivity and compete with target-binding reactions.
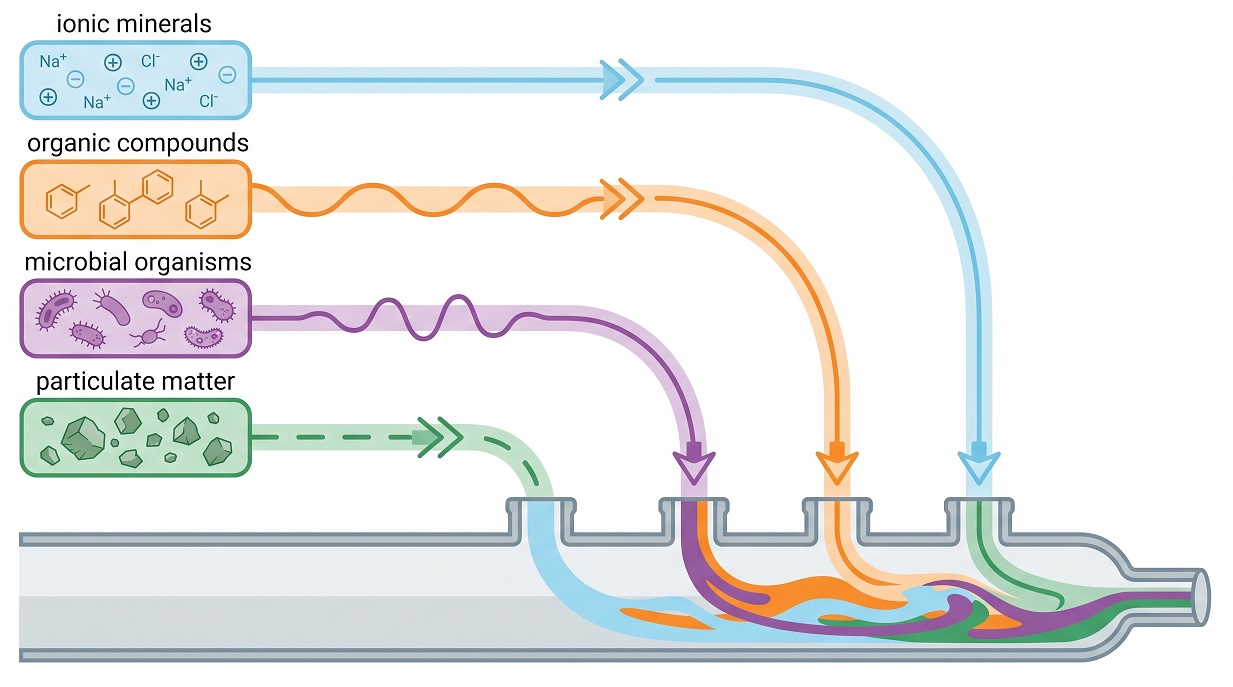
Organic compounds, measured as total organic carbon or TOC, introduce background signal in staining workflows and can inhibit enzyme-based amplification.
Microbial contamination introduces living organisms and persistent byproducts: endotoxins (fragments of bacterial cell walls) and nucleic acid-degrading enzymes. Particulate matter blocks fine instrument channels and scatters light in photometric measurements.
Why Shared Supply Water Cannot Be Controlled
That is the problem with shared lines. Shared facility water or municipal supply introduces all four contamination categories in ways a laboratory cannot monitor or correct at the point of use.
Total dissolved solids vary with seasonal source water changes and upstream treatment adjustments.
Chloramine residues from municipal disinfection are not reliably removed by standard building filtration and are known to degrade certain reagent formulations. Microbial load in shared distribution lines fluctuates with usage patterns and pipe condition, neither of which a laboratory controls.
Note: Standard building filtration is not designed to remove chloramine residues from municipal supply water. Laboratories relying on shared lines have no reliable point-of-use mechanism to correct this before it reaches reagent preparation.
The Four Parameters That Define Water Fitness
Standards bodies define fit-for-purpose laboratory water using four measurable parameters. Resistivity, expressed in MΩ·cm, reflects ionic purity. TOC, measured in parts per billion, indicates organic contamination load.
Microbial count, reported in colony-forming units per millilitre (CFU/mL), tracks biological load. Particulate content is defined by passage through a 0.2 µm rated filter.
Together, these four parameters provide an objective basis for assessing any water source or purification system.
Water Purity Demands Across Pathology Workflows
Not every section of a pathology laboratory requires the same grade of water. The purity threshold for a molecular diagnostics workflow is set by different failure modes than the one for histology, and what causes a problem in flow cytometry will not necessarily affect a cytology preparation.
A single shared supply cannot meet these distinct requirements reliably.
Where Ionic Contamination Causes Visible Artifacts
Antigen retrieval unmasks target proteins for antibody binding and requires buffer solutions prepared with ultrapure water. ASTM Type I water is the accepted standard: resistivity approaching 18.2 MΩ·cm, TOC below 10 parts per billion.
Ionic contamination above threshold alters buffer pH and conductivity, producing staining artifacts in the finished slide.
DAB chromogen development, the step that deposits brown reaction product at antibody binding sites, is sensitive to the same ionic variables. Residual mineral ions in wash solutions cause non-specific background deposits that obscure the target signal.
Ionic contamination above threshold alters buffer pH and conductivity, producing staining artifacts in the finished slide.
Why PCR Demands More Than Ionic Purity
Polymerase chain reaction (PCR) and next-generation sequencing require water that goes beyond ionic purity. Nuclease-free water, certified free of DNase and RNase (enzymes that degrade nucleic acid targets), is a minimum requirement.
Bacterial endotoxins can inhibit polymerase activity and introduce amplification variability that ionic purity measures alone do not detect. CLSI EP18-A2, the standard addressing interference testing in molecular applications, documents these thresholds.
How Wash Water Affects Cell Morphology
Liquid-based cytology preparations use wash solutions that contact cells directly. Residual minerals in those solutions alter osmotic conditions around the cell membrane, causing morphological distortion that affects diagnostic interpretation.
Organic compounds in the wash water contribute to background deposits that reduce contrast between cellular detail and slide background.
Particulates and Endotoxins in Cell-Based Assays
Flow cytometry measures light scatter and fluorescence at the individual cell level, which makes it sensitive to particles that would pass undetected in other workflows. Particulate contamination above 0.2 µm generates false scatter events that distort population gating.
Bacterial endotoxins in the sheath fluid interfere with viability markers, producing elevated dead-cell counts in cell-based assays.
Water Grade Requirements by Workflow
The purity gradient across these workflows maps directly to the water grade classifications used by standards bodies. The table below summarises the minimum grade required for each application and the primary contamination risk if that grade is not met.
| Workflow | Minimum Grade | Primary Risk if Unmet |
|---|---|---|
| Histology / IHC | ASTM Type I (18.2 MΩ·cm, TOC <10 ppb) | Staining artifacts, inconsistent antigen retrieval |
| Molecular diagnostics (PCR, sequencing) | Nuclease-free, endotoxin-controlled (beyond CLRW) | Amplification inhibition, false negatives |
| Liquid-based cytology | ASTM Type II / CLRW minimum | Cell morphology distortion, background deposits |
| Flow cytometry | CLRW with 0.2 µm filtration | False scatter events, viability marker interference |
Regulatory Requirements for Pathology Laboratory Water
Water quality is not a discretionary standard in an accredited pathology laboratory. CAP, CLSI, and ISO 15189 each address it through different mechanisms, and together they create a compliance framework that shared or municipal supply water routinely cannot satisfy.
What CAP Inspections Require on Water
The College of American Pathologists (CAP) Laboratory Accreditation Program requires documented water quality testing and records available at biennial inspection. A deficiency citation requires formal corrective action, documented remediation, and a review of reports potentially affected.
Such citations also trigger a mandatory results review to determine which patient reports fall within the affected period.
CLSI CLRW Thresholds and Their Limits
The Clinical and Laboratory Standards Institute (CLSI) Clinical Laboratory Reagent Water standard defines four minimum thresholds: resistivity greater than 10 MΩ·cm, TOC below 500 ppb, bacterial count below 10 CFU/mL, and particle filtration to 0.2 µm. These values represent the floor, not a target.
CLSI explicitly notes that CLRW may be insufficient for certain analyzer feeds, placing the confirmation obligation on each laboratory.
Important: CLSI explicitly notes that CLRW may be insufficient for certain analyzer feeds. Each laboratory carries the obligation to confirm water fitness against its instrument manufacturer specifications.
How ISO 15189 Frames Water Quality
ISO 15189, the international standard for medical laboratory quality management, treats water as a reagent input subject to documented performance monitoring and traceability requirements. Any input that affects result validity must be controlled, qualified, and recorded.
Water that is not monitored against defined parameters fails this requirement regardless of its apparent source quality.
What an Audit Finding Costs in Practice
Not all of these obligations carry equal weight in practice. A water-related audit finding carries consequences beyond the citation itself.
The corrective action burden is substantial: root cause must be established, remediation demonstrated, and affected results reviewed. For an accredited facility, a pattern of water-related findings creates reputational risk beyond a single inspection cycle.
Operational Continuity and Water System Reliability
Water quality events do not announce themselves in advance.
By the time a resistivity or TOC alarm fires mid-session, some work may already be compromised.
The Cost of a Mid-Session Water Event

Every batch processed since the last verified in-specification reading enters mandatory review when out-of-spec water is detected. Under ISO/IEC 17025, which governs testing laboratory competence, and good laboratory practice (GLP) frameworks, corrective action requires root cause investigation, remedial records, and a release decision on affected results.
Staff time consumed by this process routinely exceeds what preventive maintenance would have required.
How Dedicated Systems Prevent the Failure
Dedicated water systems reduce this risk through design rather than monitoring alone. Constant-velocity recirculation loops keep water moving continuously, preventing the stagnation conditions that allow biofilm to establish.
Ultraviolet sterilization at 254 nm inactivates bacteria in the distribution loop before they reach the point of use. Point-of-use filtration at 0.22 µm provides a final particulate barrier.
Real-time resistivity monitoring with configurable alarm thresholds flags deviation before a full session is affected.
Tip: Real-time resistivity monitoring with configurable alarm thresholds allows a laboratory to catch water quality deviation before it affects an active run, rather than discovering it during batch review.
Biofilm Risk in Shared vs Dedicated Lines
Shared distribution lines carry a different risk profile. Intermittent use creates periods of stagnation between draws, which is when bacterial biofilm colonizes pipe surfaces.
A continuously recirculating dedicated loop has no idle periods, removing the primary condition for its accumulation.
The Cost of Water System Failure in Pathology
The capital cost of a dedicated water system is the number most likely to appear in a procurement conversation. It is rarely the most relevant number.
A more useful frame is the cumulative cost of not having one.
Why Purchase Price Is the Wrong Metric
Total quality cost modeling sets rejected runs, reagent waste, repeat labor, and turnaround delay penalties against the purchase price. In a high-throughput department, recurring inadequate-water costs often exceed the annualized capital cost of a dedicated system.
What a Single Batch Failure Actually Costs
A single contamination event in an immunohistochemistry or immunofluorescence workflow carries a traceable cost structure. An invalidated batch means repeat tissue processing, delayed reports, and a CAP deficiency review.
Each element carries a staff time and reagent cost that compounds when the event recurs.
How PT Failures Accumulate Into Accreditation Risk
Proficiency testing (PT) performance is a consequential dimension that often goes untracked. Water-related assay failures that persist across testing cycles degrade PT scores in a pattern reviewers can identify.
A laboratory with a pattern of such failures faces a higher evidentiary burden at its next accreditation review.
Water System Selection as a Quality Management Decision
A dedicated water system purchased on specification alone is likely to be under-specified. Procurement tends to focus on output volume and footprint, while the questions that determine fitness get addressed later.
Starting from quality management rather than capital budgeting changes what gets asked.
Building the Argument From Evidence, Not Specification
The argument for a dedicated system does not depend on manufacturer claims. CAP, CLSI, and ISO 15189 each frame water as a controlled pre-analytical input, not a utility.
Peer-reviewed laboratory science supports the same position across histology, molecular diagnostics, and cell-based workflows. That is a different kind of evidence base than a product brochure.
Four Questions Before Committing to a Pathology Laboratory Water System
Upfront cost deserves direct acknowledgment. A centralized system for a high-throughput facility typically falls in the $20,000–$40,000 range, depending on capacity. Within a total quality cost model, that figure becomes a comparison point rather than a ceiling.

Before specifying a system, four questions are worth answering. Which workflows require which purity grade? What monitoring and documentation does each grade require under the applicable accreditation standard?
What service contract and validation protocol apply, covering installation qualification (IQ), operational qualification (OQ), and performance qualification (PQ)? And does it scale if the test menu changes?
Connect the Infrastructure Decision to Patient Safety
Water quality in a pathology laboratory is not a facilities management question. Antigen retrieval, PCR, and flow cytometry each depend on water that meets a defined purity specification.
When those standards are not met, the consequences are diagnostic, not just operational.
The regulatory framework is already in place. CAP, CLSI, and ISO 15189 each provide an independent basis for the requirement. What remains is framing the investment correctly: as a pre-analytical control rather than a capital line item.



